I have both OA and PsA through out my body, is there some way to tell which pain is coming from which disease? I mainly say this because it would be nice to tell if the biologics are working. I am seronegative on my blood work, PsA mainly manifests as Enthesis in my hands, feet legs, spine, neck, arms. Etc. OA is in my hands, feet, knees, spine elbows, shoulders and neck… I have a few Vertebrea that are fusing, mostly in my Throasic and cervical spine, and my SIJ’s are fusing. So it is hard to tell if the biologics are working, because of the damage that I already have.
My new Rheumy, who specializes in PsA, she was part of the GRAPPPA convention of Rheumatologist around the world, looking into PsA, she has papers on it etc. She was so mad at my previous Rheumy’s one of which I was with 2 years, and never took notes, so when I left the practice, they just made stuff up. She was mad at my last Rheumy for not doing the TB blood work before starting Remicade, we have since checked it, and it is fine. She finally pushed all the papers out of the way and said “lets start over” she did a exam, and didn’t find much disease activity, then she reminded herself that I am on biologics… She ordered x-ray of my hands and SIJ, it was interesting that the radiologist stated “no indication of PsA” on the report, I got a copy and found 30 indications, new bone growth from enthesis in the fingers, and 3 clear places of erosion, exactly where the Ulrasound imaging indicated. The OA was clearly visible, so maybe he stopped with that finding. I have no idea why he didn’t see the other glaring indications. I have not gone over this with my Rheumy, but it will be interesting if she notices it. I have one of the x-ray images on my computer monitor, my doctor friend was visiting, he was across the room and said, “I can see the erosion from here”…
Sorry for the long winded thread, just catching up…
John Sparky, welcome back! And a big congratulations on finding a doctor who knows her stuff and is prepared to examine you very very carefully, and is willing to put that knowledge to work. It’s shockingly common for PsA patients to be treated like you have been in the past: my first rheumatologist judged my disease as “mild”. When I went to PsA experts, they judged me as “Severe, with a lot of damage”. Go figure. You must be so glad to have the doctor you do now.
To be honest, I don’t think you can distinguish between the two kinds of pain. Tendinitis and enthesitis is outside the join, and more of a generalized achy tenderness. OA (wear and tear damage of the joint) feels the same as PsA damage of the joint. I’ve often seen it said that people have OA as a result of PsA. And I guess it doesn’t really matter.
Wow, good for your doctor, noticing the details like those fuzzy little bony outgrowths. On my first round with my PsA experts, there was some discussion between two of them about whether I had RA or PsA. (I have a low RA factor.) The top expert pointed to an x-ray of my foot and said “See that there?” It was a fuzzy little outgrowth like yours. “PsA,” he said. “RA never does that. This is PsA.”
Hi, actually I have not seen the Rheumy about this x-ray, I always get my own copy and mark it up for the next vist. I visit the radiology sites for info, I noticed the fuzzy signitures and found out it was shaft periostitis. I will let my doctor assess it, and see if she caught it, if she has, she gets all the credit! It is a shame the Scripps La Jolla Radiologist missed the new bone growth and joint erosion… Maybe it was a Friday before a 3 day weekend that distracted him?
Depends on where the “new stuff” is. If its the middle and end finger joints (called the proximal and distal interphalangeal joints) even with erosions, it’s likely OA or EOA. EOA is somewhat controversial in that many believe it is progressive and eventually becomes RA. The only way to know sure is by the shape of the erosions, which may be what the radiologist is referring to. psA erosions in the hands are generally pretty distinct in shape. If you can I’d plot your ANAs, ESRs, and CRPs for the last few years and see what the trend is. Most newer Rheumies don’t care what the norms are, they want the slope.
If the membership wants I can do a quick tutorial on how to do this with Excel to save a lot of time. ( There are free versions available) or Google sheets, I can make Excel walk and talk and on occasion sing and dance, but sheets gets me.
Shaft periostitis is a common finding, and would point to either age, athltics, orcOA. Most commonly it a stress injury, or left from a infection (usually a congenital STD). The most common shat periostitis is called shin splints. Wanna see a mess you should look at my daughter’s images. She was a pro tour tennis player. She’s fine now but her day is coming. She just had a pool installed in back yard to kkeep things moving.
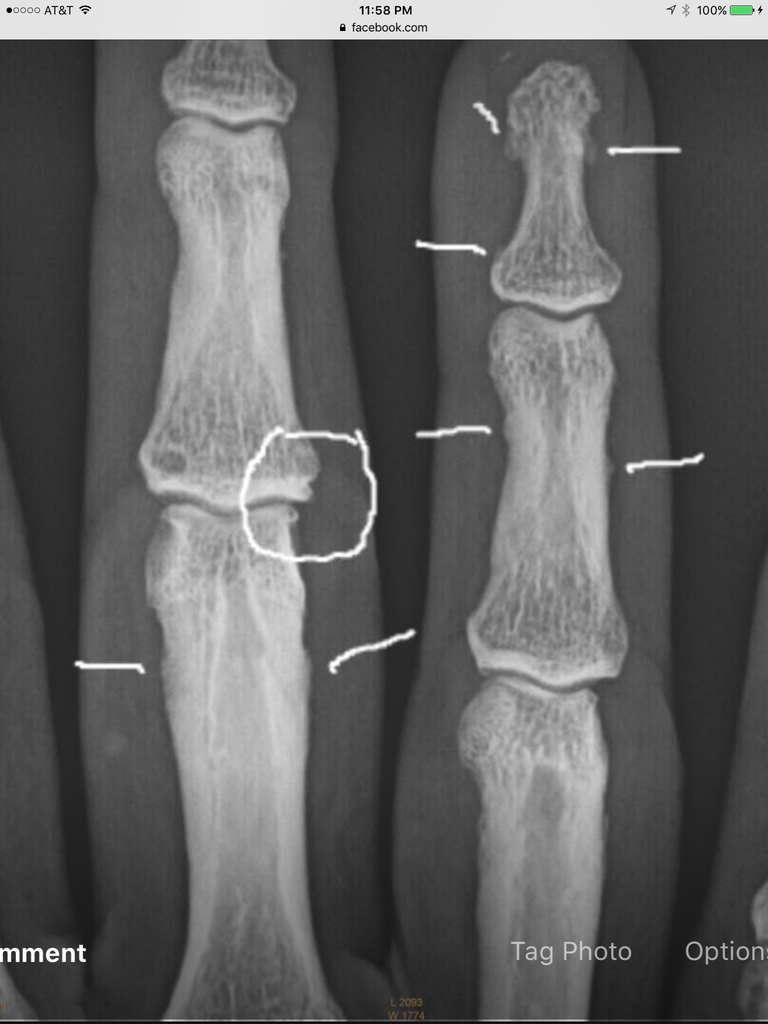
Did you see the image above of the X-ray of my hand, I circled the erosion. I have already been Dx’d with PsA, my Rheumy is leaning toward a additional overlap of AS. I read that they are now finding OA with enthesis, so you may be right… the ultrasound imaging showed Synovitis, and enthesis in these areas.
The US report stated: "erosive changes of the right third PIP, with loose body, erosive changes of the left prximal triquetrum. Small eroded surface of the proximal lunate, right and left; erosive changes of the left thirdmetacarpel head. Bilateral synovial thickening in the wrists, right third PIP, MCP’s 2 and 3 without hyperemia."
Does the “without hyperimia” signify that it is OA rather then PsA? Or that it is not currently inflamed?
I will look at my old blood tests and see if I can get the info to graft the changes, in the inflammation markers.
I also had a nuclear bone scan that showed a lot of inflammation, it was checking for cancer, so they didn’t make any comments about it, other then saying that no bone cancer was present…